
05. tbl. 102. árg. 2016
Demodex folliculorum a hidden cause of blepharitis
Demodex folliculorum, hársekkjamítill, dulin orsök hvarmabólgu
Abstract
Meibomian gland dysfunction (MGD) is a common cause of dry eye disease. Demodex mites can cause MGD with symptoms like itching, dryness and general ocular discomfort. It is important to consider infestation with Demodex mites in individuals who are non responsive to traditional MGD treatment but also equally important when cylindrical dandruff is seen at the base of the eye lashes.. We report two individuals who had not responded to ocular and systemic treatment for MGD and were then diagnosed with Demodex mites. Treatment with BlephEx and Tea tree oil was successful. This is the first report on Demodex folliculorum in Iceland where a genetic analysis was done.
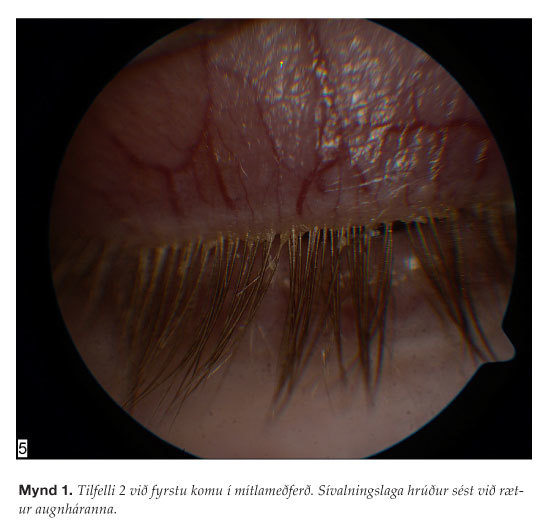
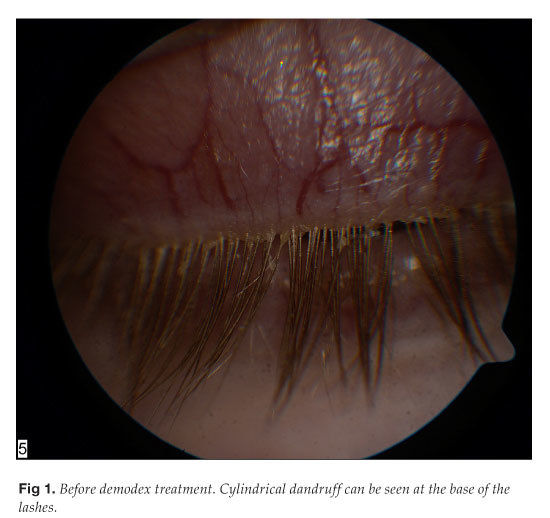
Fig 1. Before demodex treatment. Cylindrical dandruff can be seen at the base of the lashes.
{kind=link}
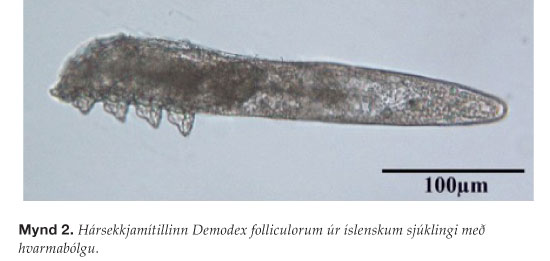
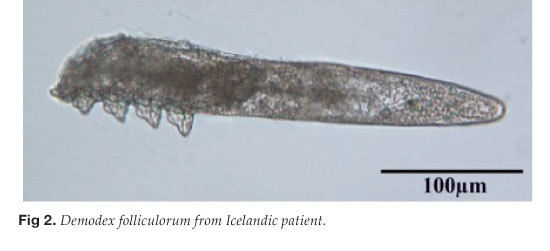
Fig 2. Demodex folliculorum from Icelandic patient.
{kind=link}
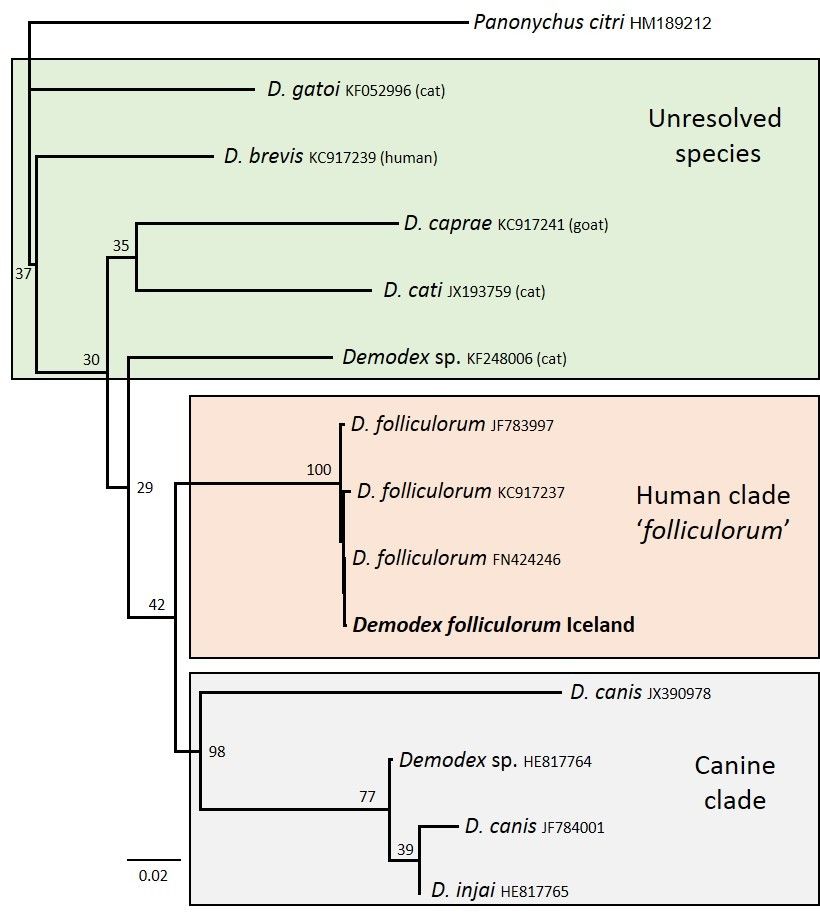
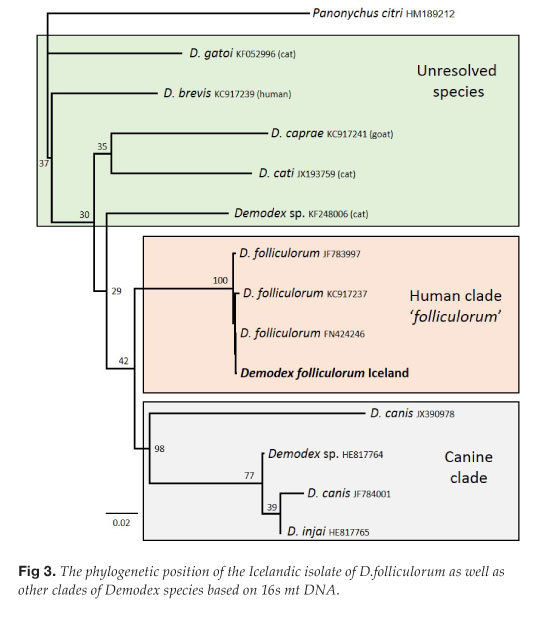
Fig 3. The phylogenetic position of the Icelandic isolate of D.folliculorum as well as other clades of Demodex species based on 16s mt DNA.
{kind=link}
Fig 4. Ten weeks after the first demodex treatment.
{kind=link}
Meibomian gland dysfunction is a common cause of dry eyes. Demodex mites may cause this type of dysfunction and, consequently, blepharitis accompanied by pruritus, dryness and general discomfort in the eye area. It is important to consider Demodex mites during diagnosis of blepharitis and in cases where conventional treatment options for blepharitis fail. Two people had received conventional treatment for blepharitis and dry eyes without any benefits and were consequently diagnosed with Demodex folliculorum. Treatment proved effective using BlephEx and Tea Tree oil. This is the first time that diagnosis of Demodex folliculorum has been confirmed with a genetic typing assay in Iceland.
Dry eyes are a common problem and studies have shown that this condition affects 5-30% of people over the age of fifty.1 The causes of dry eyes are multiple but two of the most common ones are that they are (i) aqueous deficient and (ii) evaporative, which can generally be traced back to blepharitis. The most common cause is meibomian gland dysfunction. Environmental factors, such as air humidity, are also a great influence and in many cases the cause is a combination of these factors.1
Dry eyes lead to changes in the composition of the tear film of the eye as well as on its surface, and the main symptoms are general discomfort in the eye area, vision disorders, burning sensation and the sensation of a foreign object in the eye. Conventional treatments for dry eyes include artificial tears, punctual plugs, allergy tablets and drops, oral doxycycline, steroid drops and cyclosporin eye drops. In isolated cases, this treatment has not been sufficient.
The following describes the cases of two individuals seeking medical help for dry eyes, where conventional treatments did not prove efficient. Consequently there was a rising interest in examining further whether the cause could be traced back to Demodex mites. As far as the authors of this article are aware, no such cases confirming mites by typing assay have been described in Iceland before.
Medical history
Case 1: A 72 year old male with blepharitis and persistent ocular pruritus, but otherwise healthy. Without medication but using artificial tears (Thealoz) two or three times per day for both eyes. The man complained about epiphora, foreign object sensation and ocular pruritus, despite using artificial tears.
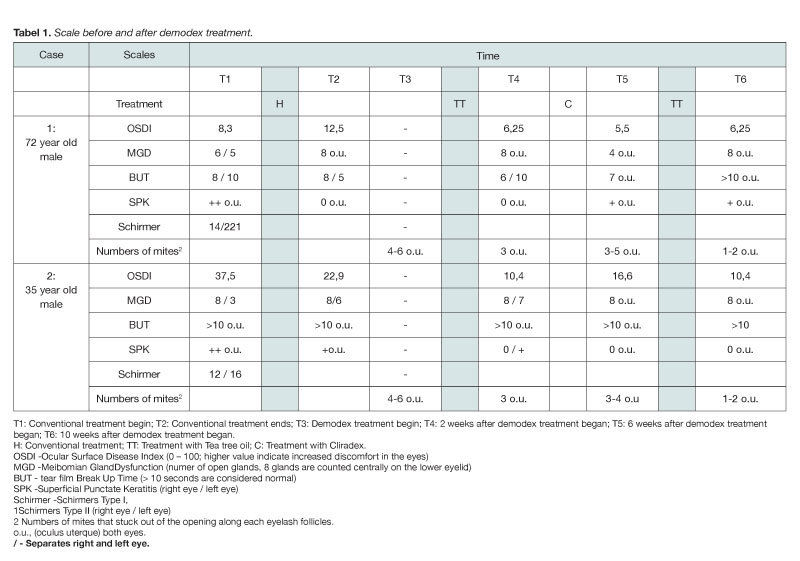
In the beginning of the conventional treatment, the patient was asked to answer a questionnaire, OSDI (Ocular Surface Disease Index), indicating the degree of ocular discomfort (high values indicate increased ocular discomfort). The conclusions of the questionnaire indicated rather little discomfort despite complaints. An examination revealed meibomian gland dysfunction and dry cornea (see column T1 in table I ). Cylindrical dandruff were also visible on eyelashes on both sides.
{kind=link}
Conventional treatment was used for 8 months and during that time various treatments were given, such as eye drops with dexametasone and tobramycin (Maxidex and Tobradex), hydrocortisone eye suspension (Hydrocortisone with Terramycin and Polymyxin B), chloramphenicolum eye ointment and doxycycline in tablet form. The need for cleaning eyelashes and using warm compresses on eye lids in the evening and morning was strongly emphasised.
Following conventional use (see column T2 in table I ), the patient still complained about itchy and dry eyes. Cylindrical dandruff were still visible on eyelashes despite repeated cleaning.
Case 2: A 35 year old healthy male without medication, with persistent pruritus and dry eyes for several years. With known blepharitis since 2009 and using artificial tears (Thealoz) three to seven times per day due to this.
Before conventional treatment (see column T1 in table I ), the OSDI results indicated a great discomfort in eyes. Examination revealed meibomian gland dysfunction as well as visible cylindrical dandruff on the eyelashes of both eyes.
Treatment was started with doxycycline in tablet form and with eye drops containing dexametasone and tobramycin (Tobradex). He also received plugs in both tear ducts, as well as instructions about cleaning eyelashes and using warm compresses on eyelids in the evening and morning.
After 5 months, the patient still complained about dry eyes and pruritus around the eyes (see further in T2 in table I ). Cylindrical dandruff were still visible on eyelashes despite repeated cleaning.
Since conventional treatment did not have the desired effect in either case and cylindrical dandruff was still visible on eyelashes, blepharitis caused by Demodex mites was soon suspected.
Studies have shown that cylindrical dandruff on eyelashes is associated with all clinical cases of Demodex infections, but the cylindrical dandruff is thought to be composed of lipids, keratin and waste products from mites.2
Examination of eyelashes with a slit lamp (magnified x25) revealed little transparent “studs” that stuck out of the opening of the eyelash follicles next to each lash, when eyelashes were pulled and turned. The more the eyelash were turned, the longer the “studs” became, and some even separated from the eyelash. Therefore, eyelash samples were collected and sent for examination to The Institute for Experimental Pathology of the University of Iceland, Keldur, where they were examined with regards to mite infection.
Mite diagnosis
The presence of Demodex mites in the samples was studied in two ways: (i) A visual examination, with stereomicroscopy and microscopy of the samples (magnified x60 – x300); (ii) A genetic study. The genetic material from the samples was isolated using a GeneMATRIX Tissue DNA purification Kit (EURx, Poland), according to instructions from the manufacturer, but the methodology of Milosevic et al.3 was applied for the PCR, using genetic markers that are specifically bound to the 16s component of mitochondrial DNA (16s mtDNA). The PRC products were sent for a sequence analysis to First BASE Laboratories Sdn Bhd in Malaysia. A BLAST (Nucleotide Basic Local Alignment Search Tool) was used for each amplified oligonucleotidic sequence, to confirm its type and evolutionary status.
During sample microscopy, mites were confirmed matching the description of Demodex folliculorum ( figure 2 ). The PRC of all samples delivered a 332 base pair product that, according to sequence analysis and comparison with known oligonucleotidic sequences, turned out to be Demodex folliculorum in all cases. Genetic equivalence with known Demodex folliculorum oligonucleotidic sequences was extensive in foreign studies, in the range of 99.5-100%. However, there was only 79% equivalence with Demodex brevis, which still has an uncertain evolutionary status as well as other Demodex species that are found in mammals ( figure 3 ).
{kind=link}
{kind=link}
Demodex mite treatment
Following these results, both individuals were offered treatment against Demodex mite infections. Before the onset of treatment, the eyelashes were photographed (see figure 1 ). Three eyelashes were inspected on each eye and the number of mites (“studs”) sticking out of each eyelash follicle were counted (see column T3 in table I ). Treatment was started by removing cylindrical dandruff from eyelashes with an electric brush (BlephEx - Rysurg, USA).
{kind=link}
Both individuals received Tea Tree wet wipes (Tea Tree Cleansing Wipes, The Body Shop) intended for the cleaning of eyelashes, eyebrows and face, in the evening and morning for two weeks. Tea tree oil contains 4-Terpineol, which kills Demodex mites.⁴ They were also advised to increase the use of artificial tears as needed and rinse eyes if they got in contact with wet wipes.
Follow-up visits
Case 1: After two weeks (see column T4 in table 1 ), the OSDI score had decreased and according to the patient “pruritus had mostly resolved”.
Cylindrical dandruff were still detectable on eyelashes of both eyes and was removed with a BlephEx electrical brush. Since no side effects appeared to be associated with the use of wet wipes, a decision was made to change to wet wipes with a higher concentration of 4-Terpineol (Cliradex Bio tissue, Doral, FL 33122, USA), than the Tea Tree wet wipes. It was recommended to use the Cliradex wipes on eyelashes, eyebrows and face, in the evening and morning for four weeks.
Six weeks after the first mite treatment (see column T5 in table I ) it was revealed that wet wipes had been used twice daily for two weeks and once daily during the third week, after which their use had been discontinued due to a burning sensation in the skin and around the eyes. Examination revealed increased cylindrical dandruff on the eyelashes of both eyes. The patient mentioned having dry eyes in the morning and occasional pruritus. Following these results a decision was made to change back to Tea Tree wet wipes and they were recommended for use in the evening and morning for four weeks. An adjuvant treatment was also administered, using doxycycline in tablet form and dexametasone eye drops for one month.
Ten weeks after the first mite treatment, the patient reported that his eyes felt comfortable and the pruritus had resolved. Eyelashes were clean and there was no visible cylindrical dandruff. The mite count results (see column T6 in table I ) suggested a reduced number of mites. It was recommended to continue using artificial tears without preservatives as needed, as well as using Tea Tree oil wet wipes in the evening and morning.
Case 2: Two weeks later the pruritus had resolved and, according to the patient, his eyes had not been this comfortable for a long time. The OSDI score supported the patient's testimony regarding a better comfort (see T4 in table I ) and, additionally, he had reduced the use of artificial tears to once daily. Slight cylindrical dandruff was detected on the eyelashes of the left eye and therefore a second BlephEx cleaning was performed on that eye. The Tea Tree wipes did not cause any side effects and therefore a decision was made to change to Cliradex wipes that were to be used for four weeks, in the evening and morning, on eyelashes, eyebrows and face.
Four weeks later (six weeks after the first mite treatment, see column T5 in table I ) it was revealed that wet wipes had hardly been used since their use was accompanied by a burning sensation in face and around the eyes. The patient claimed that his eyes felt worse and he had increased the use of artificial tears to three times daily. Cylindrical Dandruff had increased around eyelashes on both eyes. Both eyes were cleaned with BlephEx and then treatment was continued with Tea Tree wipes, evenings and mornings for four weeks.
Ten weeks after the first mite treatment (see column T6 in table I ) the patient felt comfortable in and around the eyes and no pruritus was present. Eyelashes were clean ( figure 4 ) and mite count indicated a reduced number of mites. The patient was discharged and advised to continue using artificial tears without preservatives as needed and Tea Tree oil wet wipes in the evenings and mornings.
{kind=link}
Conclusions/Discussion
Demodex folliculorum causes blepharitis with associated symptoms.
Treatment with Tea Tree oil wet wipes is effective. Cleaning eyelashes with BlephEx provides a good adjuvant treatment since it seems to be difficult for patients to adequately clean the cylindrical dandruff off eyelashes at home.
The authors are not aware of any previous studies regarding blepharitis caused by Demodex mites in humans in Iceland.
Mites become more common with increasing age and 84% of all individuals aged 60-70 are believed to have Demodex mites, and 100% of those who are 70 and older.5 The number of mites on each individual are believed to be in the range of 1000 to 2000.2
Demodex mites were first discovered by the anatomist Jacob Henle in 1841 and a year later the first species, Demodex folliculorum (the hair follicle mite), was described.6 Today, there are at least 86 species known of the Demodex genus, two of which are found in humans: Demodex folliculorum and Demodex brevis.7 The two species use different food sources and the first type is mostly found within the eyelash follicles, where several mites often reside together, whereas the latter type resides quite deep inside lipid glands (sebaceous glands and meibomian glands) and generally only as a single mite.8,9
Fully grown Demodex folliculorum mites are approximately 0.3-0.4 mm long but Demodex brevis are a bit shorter, approximately 0.15-0.2mm, and both species are therefore invisible to the naked eye. The mites are almost transparent and stud-shaped, with four pairs of legs on a short front body and a long cylindrically shaped back body. The mite life-cycle is aproximately 15 days. Mating takes place in the top part of the follicle, after which the fertilised female moves downwards inside the follicle (D. folliculorum) or into the lipid gland (D. brevis) where it lays its eggs. It takes approximately 12 hours from mating until eggs are laid and 60 hours later larvae are hatched from the eggs. Following this, there is a 6 day development process, including a few larva stages, until an adult being has fully developed. The lifetime of adult mites is believed to be approximately one week. Everything indicates that contamination between humans happens with direct contact, since the mites only survive for a very short period outside the host.6,8,9
Demodex folliculorum and Demodex brevis are generally believed to be harmless symbionts of the skin 10 but when their numbers are greatly increased (demodicidosis) they can cause various skin diseases as well as blepharitis.5,6,10
The mites are believed to feed off epicytes in follicles and lipid glands, which then leads to dysfunction and therefore imbalance in the lipid layer of the lachrymal membrane and inflammation on the surface of the eye. It is also believed that mites and their products activate the host's immune system with an associated inflammation response.11 Most mites die inside eyelash follicles and lipid glands. There they resolve and leave accumulated waste as well as various bacteria that they bring with them.12 Studies have shown that the lachrymal fluid of Demodex includes more of the cytokine interleukin-17 (IL-17), which induces inflammation response and obstruction in glands as well as possibly causing damage on the surface of the eye. Treatment with Tea Tree oil has been demonstrated to have a lowering effect on IL-17 values, which improves the host's comfort.13,14
It can be difficult to exterminate Demodex mites from eyelash follicles since treatment adherence is very important.14 Therefore, treatment is rather aimed at reducing the number of mites to improve the patients' comfort. Several treatments have been tried abroad; especially different types of creams that are intended to keep the mites from multiplying and Tea Tree oil (4-Terpineol) that kills them.5 Studies have also revealed that the drug Ivermectin, used to treat various parasites such as nematodes, is useful as an adjuvant treatment against Demodex infections.15 There is also evidence that indicates the benefit of brushing eyelashes with BlephEx in addition to other treatments. BlephEx is effective for cleaning cylindrical dandruff from the eyelashes as well as the microorganism membrane that is believed to cover the edges of the eyelids in those who suffer from blepharitis.16
The main symptoms of dry eyes and blepharitis are foreign object sensation, pruritus, burning sensation, discharge from eyelashes, redness on the edges of eyelids and changing vision. Pruritus and foreign object sensation are the most common symptoms of blepharitis caused by Demodex.2 Blepharitis is a common problem that responds well to conventional treatment in most cases. A lack of benefit from conventional treatment is the most common denominator for blepharitis caused by Demodex. Several individuals suffering from blepharitis caused by Demodex have tried a great number of different therapeutic treatments due to dry eyes, meibomian gland dysfunction and allergies, including artificial tears, allergy medication and drops, oral doxycycline, steroid drops and cyclosporin eye drops.
During eye examination with a slit lamp it is important to look for “stud-shaped” phenomena in the follicles along the eyelashes and they are best visible with at least a 25x magnification5. Cylindrical Dandruff (CD) at the base of the eyelashes ( figure 1 ) is symptomatic for Demodex blepharitis.17 The mites stay inside the eyelash follicles and only a little part of them is seen outside these. By pulling the eyelashes carefully with tweezers and turning them like a spoon inside a bowl, the mites are forced out into the follicle opening and will thereby become visible.11,14
These two cases showed improvement following mite treatment and described a certain relief, since pruritus was greatly reduced or resolved. The eyelashes looked much better and the OSDI questionnaire confirmed improved eye comfort. Blepharitis caused by Demodex is under diagnosed, even though its existence has been known for several years. Therefore, it is important to look for Demodex mites when cylindrical dandruff is visible on eyelashes and if conventional treatment has not proved sufficient.
Finally, it is worth remembering what Coston wrote in 1967:18 „Consider the scrambling of this microscopic octopoded mob while the host sleeps: males seeking, finding, breeding females; gravid females seeking new follicles; inhabitants of follicles sweeping feces outside.“
Acknowledgements
Dr. Halldor Palmar Halldorsson, biologist at The University of Iceland's Research Centre in Sudurnes, for recommendations and implementation of sample collection.
References
| 1. 2007 Report of the International Dry Eye WorkShop (DEWS). Ocul Surf 2007; 5: 75-107. PMid:17508116 |
|
| 2. Hom MM, Mastrota KM, Schachter SE. Demodex: Clinical cases and diagnostic protocol. Optom Vis Sci 2013; 90: e198-205. https://doi.org/10.1097/OPX.0b013e3182968c77 PMid:23748846 |
|
| 3. Milosevic MA, Frank LA, Brahmbhatt RA, Kania SA. PCR amplification and DNA sequencing of Demodex injai from otic secretions of a dog. Vet Dermatol 2013; 24: 286-e66. https://doi.org/10.1111/vde.12010 PMid:23470180 |
|
| 4. Tighe S, Gao YY, Tseng SC. Terpinen-4-ol is the Most Active Ingredient of Tea Tree Oil to Kill Mites. Transl Vis Sci Technol 2013; 2: 2. https://doi.org/10.1167/tvst.2.7.2 PMid:24349880 PMCid:PMC3860352 |
|
| 5. Liu J, Sheha H, Tseng SC. Pathogenic role of Demodex mites in blepharitis. Curr Opin Allergy Clin Immunol 2010; 10: 505-10. https://doi.org/10.1097/ACI.0b013e32833df9f4 PMid:20689407 PMCid:PMC2946818 |
|
| 6. Rufli T, Mumcuoglu Y. The hair follicle mites Demodex folliculorum and Demodex brevis: biology and medical importance. A review. Dermatologica 1981; 162: 1-11. https://doi.org/10.1159/000250228 PMid:6453029 |
|
| 7. Desch CE. Human hair follicle mites and forensic acarology. Exp Appl Acarol 2009; 49: 143-6. https://doi.org/10.1007/s10493-009-9272-0 PMid:19557529 |
|
| 8. Rather PA, Hassan I. Human demodex mite: the versatile mite of dermatological importance. Indian J Dermatol 2014; 59: 60-6. https://doi.org/10.4103/0019-5154.123498 PMid:24470662 PMCid:PMC3884930 |
|
| 9. Desch C, Nutting WB. Demodex folliculorum (Simon) and D. brevis akbulatova of man: redescription and reevaluation. J Parasitol 1972; 58: 169-77. https://doi.org/10.2307/3278267 PMid:5062457 |
|
| 10. Elston CA, Elston DM. Demodex mites. Clin Dermatol 2014; 32: 739-43. https://doi.org/10.1016/j.clindermatol.2014.02.012 PMid:25441466 |
|
| 11. Mastrota KM. Method to identify Demodex in the eyelash follicle without epilation. Optom Vis Sci 2013; 90: e172-4. https://doi.org/10.1097/OPX.0b013e318294c2c0 PMid:23670124 |
|
| 12. Bruenech JT, Haugen I-BK. Tørt øye og parasitten Demodex. Scand J Optometry Vis Sci 2014; 7: 1-8. https://doi.org/10.5384/sjovs.vol7i1p |
|
| 13. Kim JT, Lee SH, Chun YS, Kim JC. Tear cytokines and chemokines in patients with Demodex blepharitis. Cytokine 2011; 53: 94-9. https://doi.org/10.1016/j.cyto.2010.08.009 PMid:21050771 |
|
| 14. Koo H, Kim TH, Kim KW, Wee SW, Chun YS, Kim JC. Ocular surface discomfort and Demodex: effect of tea tree oil eyelid scrub in Demodex blepharitis. J Korean Med Sci 2012; 27: 1574-9. https://doi.org/10.3346/jkms.2012.27.12.1574 PMid:23255861 PMCid:PMC3524441 |
|
| 15. Holzchuh FG, Hida RY, Moscovici BK, Villa Albers MB, Santo RM, Kara-Jose N, et al. Clinical treatment of ocular Demodex folliculorum by systemic ivermectin. Am J Ophthalmol 2011; 151: 1030-4 e1. | |
| 16. Connor C, Choat C, Narayanan S, Kyser K, Rosenberg B, Mulder D. Clinical Effectiveness of Lid Debridement with BlephEx Treatment. Invest Ophthalmol Vis Sci 2015; 56: 4440. | |
| 17. Gao YY, Di Pascuale MA, Li W, Liu DT, Baradaran-Rafii A, Elizondo A, et al. High prevalence of Demodex in eyelashes with cylindrical dandruff. Invest Ophthalmol Vis Sci 2005; 46: 3089-94. https://doi.org/10.1167/iovs.05-0275 PMid:16123406 |
|
| 18. Coston TO. Demodex folliculorum blepharitis. Trans Am Ophthalmol Soc 1967; 65: 361-92. PMid:4229846 PMCid:PMC1310279 |
|