
05. tbl. 101. árg. 2015
Fræðigrein
Eating Disorder Treatment in Iceland - Treatment adherence, psychiatric co-morbidities and factors influencing drop-out
Átröskunarmeðferð á Íslandi - sjúkdómsmynd, meðferðarheldni og forspárþættir brottfalls
Objective: Treatment adherence in patients with eating disorders (ED) in Iceland is unknown. The aim of the study was to investigate treatment drop-out and explore factors that influence premature termination of treatment in a specialized ED treatment unit, at the University Hospital of Iceland, during the period of September 1, 2008 - May 1, 2012.
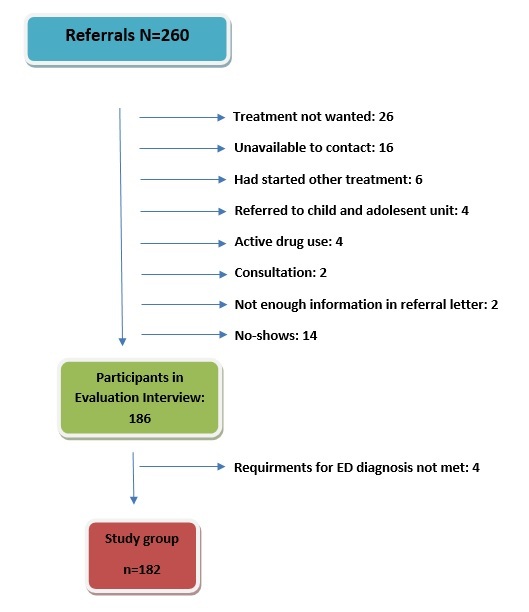
Material and Methods: The study is retrospective and naturalistic. Hospital records of referred patients were examined. Those meeting the ICD 10 criteria of anorexia nervosa (AN) (F50.0, F50.1), bulimia nervosa (BN) (F50.2, F50.3) and eating disorder not otherwise specified (EDNOS) (F50.9) were included. The total sample was 260 and 182 patients met inclusion criteria. No-shows were 7%. Drop-out was defined as premature termination of treatment without formal discharge.
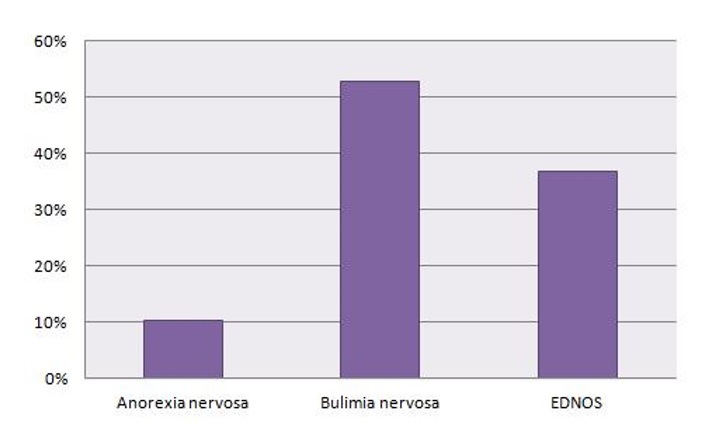
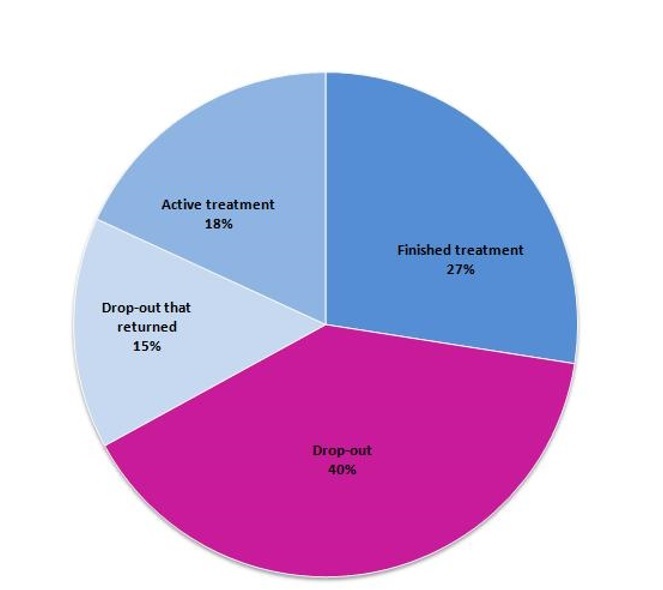
Results: The sample consisted of 176 women and 6 men, mean age 26.3 years. BN was diagnosed in 52.7% of patients, EDNOS in 36.8% AN in 10.4%. 74.7% had one or more co-morbid psychiatric diagnosis. Anxiety- and/or depression were diagnosed in 72.5%, Attention hyperactivity deficiency disorder in 15.4% and personality disorders in 8.2%. Lifetime prevalence of substance use disorders (SUDs) was 30.8%. Drop-out from treatment occurred in 54.4% of cases (with approximately 1/3 returning to treatment), 27.5% finished treatment and 18.1% were still in treatment at the end of the follow up period. Treatment adherence was significantly higher in patients who had a university degree, in those who had themselves taken the initiative to seek ED treatment and in those with higher anxiety scores at assessment. AN patients did better than other ED patients while patients with SUDs showed a tendency for higher drop-out (p=0.079).
Conclusion: The drop-out rates were similar to what has been reported from other western countries. Follow-up time was longer and AN patient did better than expected. Higher education, initiative in seeking treatment and higher anxiety scores on questionnaires were protective.
{kind=link}
Figure 2
{kind=link}
Figure 3
{kind=link}
{kind=link}
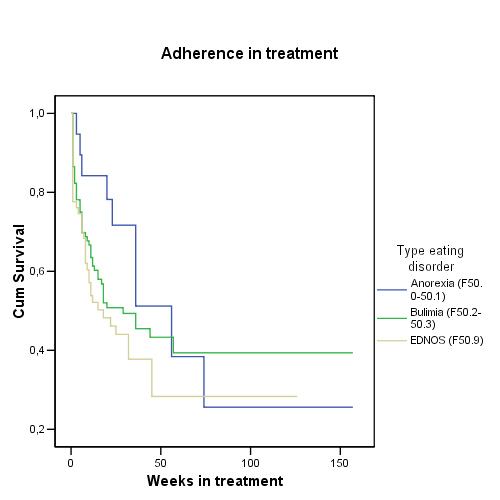
Figure 4
-The curve describes adherence by eating disorder type. Anorexia median survival time 55,6 weeks compared to Bulimia (28,6) and EDNOS (17,3).
|
Table 1. Demographic and clinical data of follow up patients (n=182). |
N % |
| Sex | |
| Female | 176 (96,7) |
| Male | 6 (3,3) |
| Body Mass Index | |
| <18,5 | 28 (15,6) |
| 18,5-24,9 | 114 (63,3) |
| 25,0-29,9 | 24 (13,3) |
| >30,0 | 14 (7,8) |
| Education | |
| Elementary School | 112 (61,9) |
| High School | 44 (24,3) |
| University degree | 25 (13,8) |
| Accommodations | |
| Lives with parents | 69 (37,9) |
| Lives alone | 27 (14,8) |
| Lives with spouse/friend | 27 (14,8) |
| Lives with family (child in home) | 59 (32,4) |
| Ethnicity | |
| Native (Icelandic) | 176 (96,7) |
| Foreign | 6 (3,3) |
| Employment | |
| Unemployed/ financial support | 57 (31,3) |
| Employed | 51 (28,0) |
| Attending school | 74 (40,7) |
| Subtype of eating disorder | |
| Anorexia Nervosa (F50.0/ F50.1) | 19 (10,4) |
| Bulimia Nervosa (F50.2/ F50.3) | 96 (52,7) |
| Eating Disorder not otherwise specified(F50.9) | 67 (36,8) |
| Comorbid psychiatric disorder | |
| Any comorbid psychiatric disorder | 136 (74,7) |
| -Anxiety / Depression disorder (F30.-/F40.-) | 132 (72,5) |
| -ADHD/ADD (F90.-) | 28 (15,4) |
| -Peronality disorder (F60.-) | 15 (8,2) |
| Alcohol/ Drug abuse | |
| Life prevalence of alcohol/drug abuse disorder | 56 (30,8) |
| -Harmful use of alcohol (F10.1) | 4 (2,2) |
| -Alcohol dependence syndrome (F10.2) | 23 (12,6) |
| -Cannabinoid dependence syndrome (F12.2) | 1 (0,5) |
| - Multiple drug use (F19.1) | 3 (1,6) |
| -Multiple drug use, dependence (F19.2) | 25 (13,7) |
| Life time prevalence of traumatic events | 144 (79,6) |
| History of suicide attempt/s | 43 (23,6) |