
11. tbl. 100. árg. 2014
Surgical outcome of mitral valve repair in Iceland 2001-2012
Objectives: To review, for the first time, the outcome of mitral valve repair operations in Iceland.
Material and methods: A retrospective study of all mitral valve repair patients (average age 64 yrs, 74% males) operated in Iceland 2001-2012. All 125 patients had mitral regurgitation; either due to degenerative disease (56%) or functional regurgitation (44%). Survival was estimated using the Kaplan-Meier method. The median follow-up time was 3.9 years
Results: The number repair-procedures increased from 39 during the first half of the study period to 86 during the latter period. The mean EuroSCORE was 12.9% and 2/3 of the patients were in NYHA class III/IV. Half of them had severe mitral regurgitation, 12% had a recent myocardial infarction, and 10% a history of previous cardiac surgery. A ring annuloplasty was performed in 98% of cases, a posterior leaflet resection was done in 51 patients (41%), 28 received artificial chordae (Goretex®) and 7 an Alfieri-stitch. Concomitant cardiac surgery was performed in 83% of cases, where coronary artery bypass (53%), Maze-procedure (31%) or aortic valve replacement (19%) were most common. Major complications occurred in 56% of the cases and minor complications were noted in 71% of cases. Two patients later required mitral valve replacement. Eight patients died within 30 days (6%) and 5-year overall survival was 79%; or 84% and 74% for the degenerative and functional groups, respectively.
Conclusions: The number of mitral valve repairs in Iceland increased significantly over the study period. Complications are common but operative mortality and long-term survival is similar to that reported in studies from other countries.
Table I. Demographics of the 125 patients that underwent mitral valve repair in Iceland from 2001 to 20012. Number of patients and % in parentheses, except for age and EuroSCORE, where means with standard deviation are shown.
|
All patients (n=125) |
Functional regurgitation (n=55) |
Degenerative disease (n=70) |
|
| Male gender | 92 (74) | 42 (76) | 50 (71) |
| Age (years) | 64 (± 14) | 70(± 9) | 60(± 15) |
| Previous cardiac surgery | 12 (10) | 8 (15) | 4 (6) |
| Hypertension | 85 (68) | 43 (78) | 42 (60) |
| Diabetes | 6 (5) | 4 (7) | 2 (3) |
| History of smoking | 69 (55) | 30 (55) | 38 (54) |
| Body mass index ≥25 kg/m2 | 81 (65) | 36 (66) | 45 (64) |
| Chronic obstructive lung disease | 19 (15) | 10 (18) | 9 (13) |
| Pulmonary hypertension (systolic pressure > 60 mmHg) | 50 (40) | 24 (34) | 26 (47) |
| Coronary artery disease | 68 (54) | 44 (80) | 24 (34) |
| NYHA class | |||
| I+II | 44 (35) | 9 (16) | 35 (50) |
| III + IV | 81 (65) | 46 (84) | 35 (50) |
| ASA* score | |||
| 1+2 | 17 (14) | 1 (2) | 16 (23) |
| 3 | 82 (66) | 37 (67) | 45 (64) |
| 4 | 26 (21) | 17 (30) | 9 (13) |
| EuroSCORE II | 5(± 7) | 7 (± 8) | 3(± 4) |
| Log EuroSCORE | 13 (± 16) | 19 (± 20) | 8 (± 10) |
*American Association of Anesthesiology
Table II. Preoperative echocardiograms of the 125 patients that underwent mitral valve repair in Iceland from 2001 to 2012. Means with standard deviation are given, except for LVESD and EF where number (%) is shown.
|
All the patients (n=125) |
Functional regurgitation (n=55) |
Degenerative disease (n=70) |
|
| Left ventricular ejection (%) | 54 ± 12 | 49 ± 13 | 58± 9 |
| Severe mitral insufficiency | 62 (50) | 48 (69) | 14 (26) |
| Left atrium diameter (mm) | 47 ± 7 | 47 ± 7 | 48 ± 7 |
| Left ventricular end-diastolic diamter (mm) | 60 ± 9 | 60 ± 9 | 60± 9 |
| Left ventricular end-systolic diameter (mm) | 41 ± 10 | 43± 10 | 40 ± 9 |
| Increased left ventricular end-systolic diameter (LVESD≥45mm) |
35 (38)
|
21 (50) | 14 (28) |
| Decreased ejection fraction (EF≤60%) | 63 (51) | 38 (69) | 25 (37) |
Table III. Short-term complications in patients that underwent mitral valve repair in Iceland between 2001 to 2012. The number of patients is shown with percentage in parentheses. Patients can have more than one complication.
|
All the patients (n=125) |
Functional regurgitation (n=55) |
Degenerative disease (n=70) |
|
| Major complications | 67 (54) | 35 (64) | 32 (46) |
| Perioperative myocardial infarction* | 21 (17) | 12 (22) | 9 (13) |
| Severe respiratory failure | 3 (2) | 3 (6) | 0 (0) |
| Tracheostomy | 8 (6) | 6 (11) | 2 (2) |
| Reoperation for bleeding | 17 (14) | 9 (16) | 8 (11) |
| Perioperative heart failure requiring intraaortic ballon pump (IABP) | 18 (14) | 11 (20) | 7 (10) |
| Acute renal failure requiring dialysis | 4 (3) | 3 (6) | 1 (1) |
| Permanent stroke | 5 (4) | 3 (6) | 2 (3) |
| Deep sternal infection | 5 (4) | 5 (9) | 0 (0) |
| Bradycardia requiring pacemaker | 6 (5) | 3 (6) | 3 (4) |
| Sepsis | 3 (3) | 2 (4) | 1 (1) |
| Minor complications | 87 (70) | 43 (78) | 44 (63) |
| New onset atrial fibrillation‡ | 29 (23) | 15 (27) | 14 (20) |
| Minor cardiac injury§ | 35 (28) | 23 (41) | 12 (17) |
| Pleural fluid requiring drainage | 33 (26) | 21 (38) | 12 (17) |
| Pneumonia | 20 (16) | 14 (26) | 6 (9) |
| Urinary tract infection | 11 (9) | 6 (11) | 5 (7) |
| Superficial wound infection | 7 (6) | 5 (9) | 2 (3) |
| Transient ischemic attack of the brain | 2 (2) | 1 (2) | 1 (1) |
| Death within 30 days from surgery | 8 (6) | 4 (7) | 4 (6) |
*Postoperative CK-MB over 70 µg/L in patients who did not have recent preoperative myocardial infarction and over 100 µg/L for patients who underwent concomitant Maze procedure
‡only including 69 patients that did not have atrial fibrillation preoperatively
§Need for inotropes >24hours after surgery
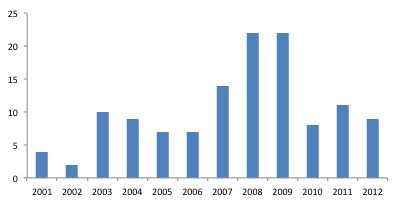
Figure 1. Annual number of mitral valve repair procedures from 2001 to 2012.
{kind=link}