04. tbl. 97. árg. 2011
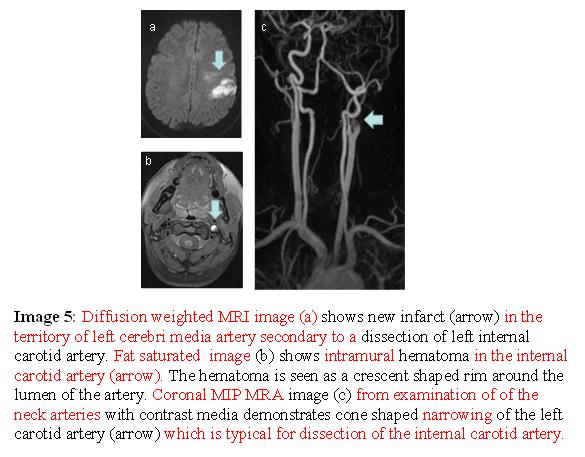
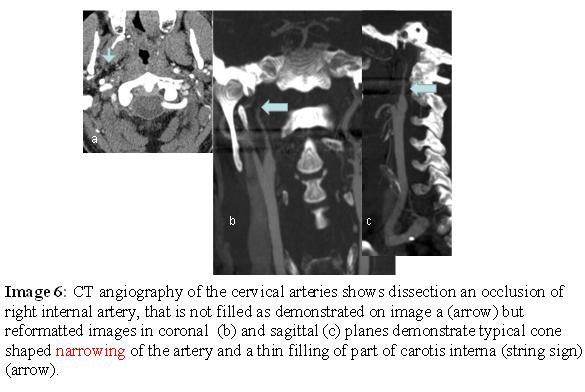
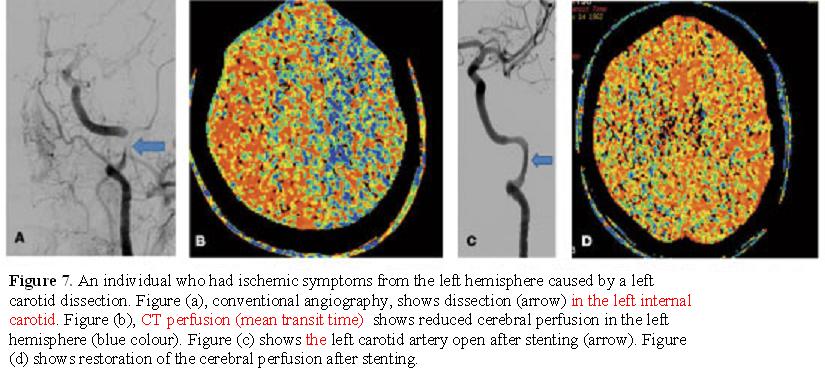
Cervical artery dissection – review
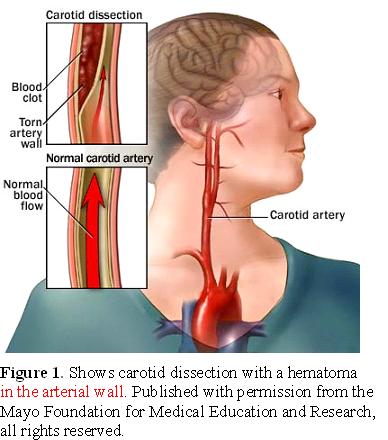
In recent years carotid and vertebral artery dissections have been diagnosed more frequently, probably because new imaging techniques are more reliable and they are certainly less invasive. The cause of cervical artery dissections is largely unexplained but probably involves a combination of genetic and environmental factors such as trauma or infection.
Most authors recommend intravenous heparin or low molecular weight heparin followed by oral warfarin to maintain INR between 2-3 for 3-6 months. If the artery has healed after 3-6 months of anti-coagulation all treatment can be stopped but if there is a remaining stenosis the patient can be put on aspirin 75-100 mg a day. The long-term prognosis of cervical artery dissection is favourable in the majority of patients. New dissections are uncommon.
SveinssonOA, Kjartansson O,Valdimarsson EM.
Cervical artery dissection – review. Icel Med J 2011; 97: 237-43
Keywords: cervical artery dissection, internal carotid artery, vertebral artery, cerebral ischemia, cerebral infarction.
Correspondence: Olafur Sveinsson olafur.sveinsson@karolinska.se
| Fibromuscular dysplasia |
| Marfan´s syndrome |
| Ehlers-Danlos syndrome |
| Autosomal dominant polycystic kidney disease |
| Osteogenesis imperfecta |
| Alpha-1-antitrypsin deficiency |
| Cystic medial necrosis |
| Type 1 collagen mutation |
| Other connective tissue diseases |
Table 1. Diseases which are known to be associated with an increased risk of cervical artery dissection.