
01. tbl. 102. árg. 2016
Transport and treatment of patients with STEMI in rural Iceland – Only a few patients receive PPCI within 120 minutes
Introduction: ST-segment Elevation Myocardial Infarction (STEMI) is a life-threatening disease and good outcome depends on early restoration of coronary blood flow. Primary percutaneous coronary intervention (PPCI) is the treatment of choice if performed within 120 minutes of first medical contact (FMC) but in case of anticipated long transport or delays, pre-hospital fibrinolysis is indicated. The aim was to study transport times and adherence to clinical guidelines in patients with STEMI transported from outside of the Reykjavik area to Landspitali University Hospital in Iceland.
Materials and methods: Retrospective chart review was conducted of all patients diagnosed with STEMI outside of the Reykjavik area and transported to Landspitali University Hospital in Reykjavik in 2011-2012. Descriptive statistical analysis and hypothesis testing was applied.
Results: Eighty-six patients had signs of STEMI on electrocardiogram (ECG) at FMC. In southern Iceland nine patients (21%) underwent PPCI within 120 minutes (median 157 minutes) and no patient received fibrinolysis. In northern Iceland and The Vestman Islands, where long transport times are expected, 96% of patients eligible for fibrinolysis (n=31) received appropriate therapy in a median time of 57 minutes. Significantly fewer patients received appropriate anticoagulation treatment with clopidogrel and enoxaparin in southern Iceland compared to the northern part. Mortality rate was 7% and median length of stay in hospital was 6 days.
Conclusions: Time from FMC to PPCI is longer than 120 minutes in the majority of cases. Pre-hospital fibrinolysis should be considered as first line treatment in all parts of Iceland outside of the Reykjavik area. Directly electronically transmitted ECGs and contact with cardiologist could hasten diagnosis and decrease risk of unnecessary interhospital transfer. A STEMI database should be established in Iceland to facilitate quality control.
Figure 1. Iceland divided into the north area including Vestman Islands (blue zone) where patients are normally transported in a air ambulance (fixed wing) and the south area (red zone) where patients are normally transported with a ambulance (car). The circles represent number of patients from each country part during a two year period and the bar chart shows STEMI incidence per 100.000 inhabitants.
Figure 2. What did the first EKG show? Blue = STEMI, Red = No signs of STEMI, Green = Not taken/not found, Purple = Difficult to interpret
Figure 3. Treatment with enoxaparin/heparin and clopidogrel were significantly different between the north area (blue) and south area (red).
Figure 4. The boxplot shows the distribution of total transportation time (from first medical contact to arrival at Landspitali University Hospital) between different areas of Iceland. One forth of values lies abowe the box and one forth below. The line across the inside of the box represents the median value. The whiskers go out to the variable‘s smallest and largest values, with the exception of outliers indicated with a circle and extreme outliers, indicated with an asterisk.
Figure 5. Flowchart and timeline of patients with STEMI depending on which treatment is provided. Organization of the health care must guarantee that each patient receives optimal care.
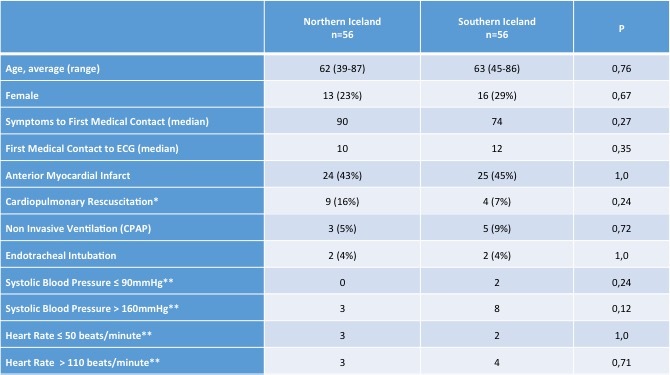
Table I. Information on patients diagnosed with STEMI at Landspitali between areas. Median times are reported in minutes. *Before arrival at Landspitali Hringbraut.**At arrival at Landspitali.
{kind=link}
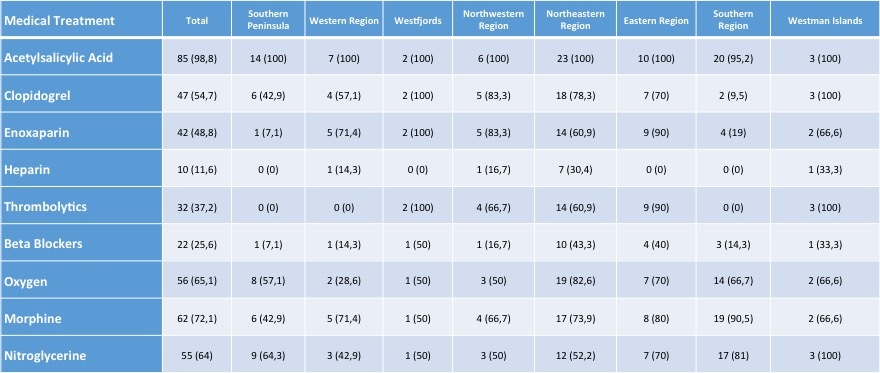
Table II. Pharmcological treatment in STEMI in different areas. Number of patients (%)
{kind=link}
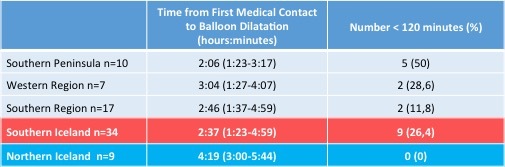
Table III. Comparison of time (median) from first medical contact to balloon inflation between different areas in patients with STEMI diagnosed rurally who underwent primary PCI and number of patients (%) with time under 120 minutes.
{kind=link}
Table IV. Number of incidents during the first 30 days from admission (%)
{kind=link}